
By Dimity McCracken
These are images from real ICU patients.
[su_tabs][su_tab title=”History”]
75yo man presented with urosepsis. After appropriate antibiotics & initial fluid resuscitation he was needing vasopressors. He had a failed insertion of R IJ CVC. Subsequently a femoral line was successfully inserted & vasopressors were started. He stabilised quickly on low dose noradrenaline.
A few hours later he became more tachycardic w dramatically increasing noradrenaline requirements. What investigation would you perform, & why?
[/su_tab][su_tab title=”Image”]

First CXR shows some R apical capping – a sign of haemothorax. The next investigation would be to repeat the CXR.
The attempted R IJ approach was very low in this case, & caused a vascular injury resulting in a massive haemothorax. Note the associated tension pushing the mediastinum to the left side.
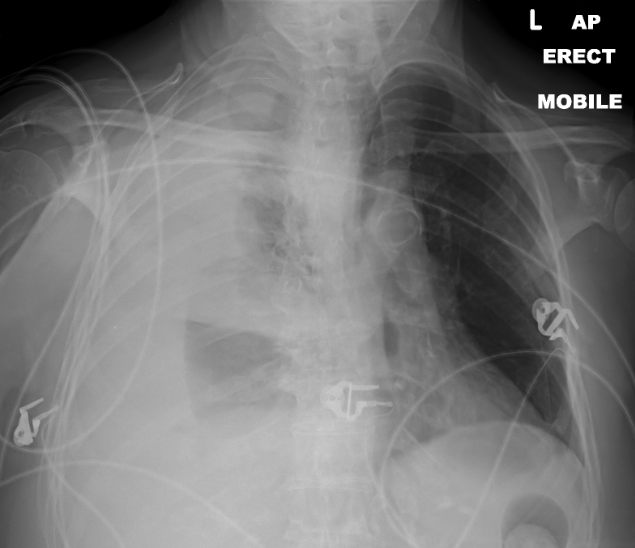
Patient subsequently required intubation, insertion of 2 chest drains, & blood product resuscitation.
This did not control the bleeding, so patient went to theatres for an emergency vascular repair.

[/su_tab][su_tab title=”Learning Point”]
For every procedure you perform:
-know the anatomy
-know the potential complications
-recognise a complication early – don’t be proud! Everyone has complications at some time or other!
[/su_tab]
[/su_tabs]








