| Subject | Question | Answer |
|---|---|---|
| nutrition | 3 methods of determining caloric intake |
|
| neurology | Advantages of the GCS |
|
| pharmacology | antibiotics contraindicated in pregnancy include | Tetracyclines, chloramphenicol |
| toxicology | Antidotes for : BDZ; B Blocker; Local Anaesthetics; Cyanide; Digoxin; Eythlene glycol; Methanol; Orgnophosphates; Lead; Iron; Isoniazid; Valproate; |
|
| infectious disease | Antifungals: classes; mechanism of action; examples; |
|
| cardiology | Aortic dissection – classification | Stanford:
|
| Respiratory | ARDS – Berlin definition |
|
| trials | ARDSNet ARMA trial |
|
| trials | Bernard trial |
|
| trauma | Blood product dosage in trauma | Plt < 50 = 1 therapeutic dose
INR > 1.5 = FFP 15mL/kg Fibrinogen < 1g/L = Cryoprecipitate 3 – 4g Tranexamic acid = loading dose 1g over 10m then 1g over 8hrs |
| neurology | Brain death – Preconditions for clinical testing |
|
| neurology | Brain death examination -cranial nerves |
|
| paediatrics | calculating weight in paediatrics | Weight = (Age + 4) x2 |
| haematology | Causes and complications of DIC |
|
| cardiac | Causes of 1st degree heart block |
|
| haematology | causes of a raised isolated APTT |
|
| endocrine | Causes of Adrenal insufficiency |
|
| neurology | Causes of brain ring-enhancing lesions include |
|
| biochemistry | Causes of HAGMA and decreased BSL |
|
| biochemistry | Causes of HAGMA and Hypocalcemia |
|
| haematology | Causes of Heinz bodies | Heinz bodies are Hb precipitates
|
| haematology | Causes of hemolytic anemia |
|
| biochemistry | Causes of hypokalemic alkalosis |
|
| respiratory | Causes of hypoxaemia include |
|
| cardiac | Causes of mobitz type 2 heart block |
|
| gastroenterology | Causes of pancreatitis | I GET SMASHED
|
| haematology | Causes of raised APTT; raised INR; raised PT and decreased fibrinogen |
|
| biochemistry | Causes of raised urea/creatinine ratio |
|
| haematology | Causes of shistocytes |
|
| cardiac | Causes of tall R wave in V1 |
|
| haematology | Causes of thrombocytopenia |
|
| trials | CESAR trial |
|
| gastroenterology | Child pugh score: Use and Components? |
|
| trauma | Classification of burns |
|
| nutrition | Clinical features of refeeding syndrome |
|
| toxicology | Clinical features of TCA OD |
|
| haematology | Clinical features of TTP |
(mnemonic FAT RN) |
| obstetric | Clinical features suggestive of severe pre-eclampsia |
|
| trauma | Clinical signs of base of skull fracture |
|
| respiratory | Clinical signs of dynamic hyperinflation in asthma |
|
| neurology | Clinical signs of intracranial hypertension |
|
| gastroenterology | Common causes of acute major haematemesis include |
|
| infectious disease | Common pathogens for CLABSI and Common skin contaminants | Pathogens:
Skin contaminants:
|
| paediatrics | Commonest causes of congenital cyanotic heart disease |
|
| nutrition | Complications of enteral nutrition include | Tube Complictions
Feed Complications
|
| gastroenterology | Complications of pancreatitis | Abdominal
Extra-abdominal
|
| neurology | Components of the CAM ICU |
|
| respiratory | Contraindications to NIV |
|
| respiratory | Criteria for ICU admission in community acquired pneumonia (and severity) | Major (either 1 of )
Minor (a least 3 of)
|
| endocrine | Criteria for SIRS | two or more of:
|
| monitoring | CVP waveform peaks and troughs |
|
| organ donation | DCD graft survival compared with donation after brain death |
|
| monitoring | DDx discrepancies in co-oxyHb Vs puls oxyHb
|
Patient A:
Patient B:
|
| biochemistry | DDx metabolic alkalosis |
|
| trials | DECRA trial |
|
| pharmacology | Define 1/2 life |
|
| pharmacology | Define anaphylaxis | Generalised type I hypersensitivty reaction in which there is widespread mast cell degranulation.It has a variable presentation |
| renal | Define dialysis | Movement of a solute from a compartment in which it is in high concentration to one in which it is in low concentration |
| renal | Define filtration fraction |
|
| statistics | Define NNT | Number needed to treat refers to the number of patients needed to be treated with an intervention for 1 patient to have a benefit. Equals 1/ ARR |
| statistics | Define relative risk reduction; absolute risk reduction |
|
| renal | Define Sieving coefficient | Ratio of concentration of a solute in ultrafiltrate compared to concentration of solute in plasma. Want it close to 1 for molecules you wish to remove |
| statistics | Define standard deviation; define variance |
|
| statistics | Define Standardised Mortality ratio | Defined as the observed mortality rate / expected mortality rate (as estimated from scoring systems such as APACHE II) |
| renal | Define ultrafiltration | Movement of solution across a semi-permeable membrane due to a transmembrane pressure gradient |
| pharmacology | Define volume of distribution |
|
| infectious disease | Define, list organisms invovled and precautions neccesary for contact, droplet and airborne precautions |
|
| renal | Definition of Akute kidney injury | Abrupt (1-7 days ) and sustained (>24 hours) decrease in kidney function. RIFLE criteria allows for AKI to be objectively and uniformly defined |
| nutrition | Definition of Cachexia is | Weight loss and skeletal muscle wasting due to illness where the body does not reduce catabolism (unlike starvation) |
| infectious disease | Definition of CLABSI |
|
| pharmacology | Definition of clearance |
|
| organisational | Definition of Level 1 ICU | Capable of providing immediate resuscitation and short-term cardiorespiratory support major role in monitoring “at risk” patients |
| organisational | Definition of Level 2 ICU | Able to provide multi-system support for critically ill patients including ventilation, RRT and invasive cardiovascular monitoring for indefinite period.If no CTS or neurosurgery – arrangement to level III ICU. |
| organisational | Definition of Level 3 ICU | Tertiary referral unit capable of providing comprehensive critical care multi-system life support for an indefinite period commitment to academic education and researchManaged by attending intensive care specialist |
| neurology | Definition of NCSE | Change in behaviour and or mental processes from baseline associated with continuous epileptiform EEG changes but without major motor signs |
| neurology | Delirium – definition |
|
| pharmacology | Describe the PD and PK of Dabigatran |
|
| pharmacology | Describe the PD and PK of Heparin |
|
| organ donation | Determination of death for DCD |
|
| gastroenterology | Diagnosis of acute pancreatitis | At least two of
|
| cardiac | Diagnosis of infective endocarditis |
|
| obstetric | Diagnostic criteria for pre-eclampsia | Hypertension (SBP >140 or DBP >90) & Proteinuria (>300mg protein in 24hr) |
| endocrine | Diagnostic criteria for SIADH |
|
| toxicology | Dialyzable drugs include |
|
| neurology | Differentials for weakness in ICU include |
|
| neurology | Disadvantages of the GCS include |
|
| cardiac | Distinguishing features between VT and wide complex SVT |
|
| organ donation | Donor criteria for DCD |
|
| pharmacology | Doses of thrombolytics in massive PE or PE with arrest |
|
| infectious disease | dosing adjustment and monitoring in renal dysfunction for aminoglycosides; penicillins; glycopeptides; carbepenems; quinolone; |
|
| toxicology | Drugs cleared via charcoal hemoperfusion | Valproate; Phenytoin; Theophylline; |
| pharmacology | Drugs that cause QT prolongation |
|
| toxicology | Drugs with potentially useful plasma levels in overdose |
|
| cardiac | ECG features of dextrocardia |
|
| cardiac | ECG features seen in PE |
|
| infectious disease | ESBL characteristics |
|
| paediatrics | ETT size in kids | Age/4 +4 |
| biochemistry | Factors that maintain a metabolic alkalosis |
|
| trials | FEAST trial |
|
| gastroenterology | Feature of glasgow/imrie score |
|
| neurology | Features and mechanism of central cord syndrome |
|
| neurology | Features of conus medullaris and cauda equina syndrome (and mechanisms) |
|
| biochemistry | Features of hypermagnesmia |
|
| pharmacology | Features of propofol infusion syndrome |
|
| statistics | Features to look for in a systematic review |
|
| neurology | Grading of SAH |
|
| trials | HACA trial |
|
| trauma | Hemostatic resuscitation involves |
|
| haematology | HITTS – Pretest probability |
Test interpretation: 0 – 3: Low; 4 – 5: Intermediate; 6 – 8: Likely |
| biochemistry | Hyponatraemia may be classified by |
|
| trials | IABP-SHOCK II |
|
| neurology | Imaging for brain death |
|
| neurology | Indications for ICP monitor |
|
| haematology | Indications for plasma exchange |
|
| toxicology | Indications for whole bowel irrigation |
Use : non absorbable polyethylene glycol solution |
| gastroenterology | Kings College criteria for liver transplant |
|
| respiratory | Light’s criteria for pleural exudate | Pleural fluid:serum ratio
|
| biochemistry | List the 3 independant variables in the Stweart approach to acid base |
|
| organ donation | Maastricht criteria to categorise DCD donors |
Only Categories 3 and 4 are suitable for DCD in Australia |
| infectious disease | Markers of severity of C. diff infection include | Clinical (fever, HD instability, peritonitis)Laboratory (WBC >15, elevated lactate or creatinine)Radiographic (colonic distension or thickening)Colonoscopic (pseudomembranous colitis) |
| respiratory | Measures to improve oxygenation |
|
| toxicology | Mechanism of paracetamol toxicity |
|
| infectious disease | Mechanisms of resistance in VRE include |
|
| infectious disease | Mechanisms that lead to vasodilatation in Sepsis include |
|
| gastroenterology | MELD score- Use? Components? |
|
| cardiac | Methods of cooling include |
|
| pharmacology | Milrinone |
|
| neurology | Modified Rankin score (mRS) used for stroke outcomes |
|
| endocrine | Myxoedema coma clinical features |
|
| infectious disease | name the organisms that are ESCAPPM |
|
| neurology | Neuromuscular junction causes of weakness include |
these typically cause a descending pattern of paralysis |
| statistics | NHMRC “levels of evidence” hierarchy (for interventions) |
|
| monitoring | O2 extraction ratio |
|
| neurology | Observations compatible with brain death |
|
| infectious disease | Organisms causing sepsis post splenectomy |
|
| trials | OSCAR trial |
|
| trials | OSCILLATE trial |
|
| respiratory | Outline measures to prevent VAP |
|
| toxicology | Overdose drugs not adsorbed by activated charcoal |
|
| statistics | Phases of drug testing are |
|
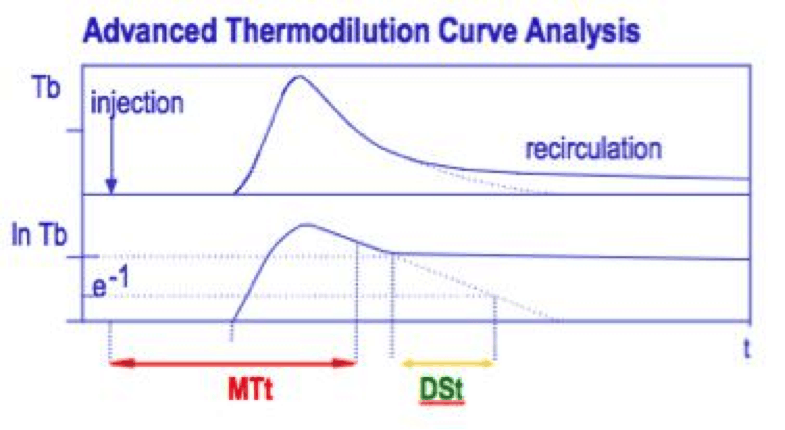
| monitoring | PiCCO: Thermodiluation volumes: GEDV, ITBV, EVLW, ITTV, PTV |
|
| paediatric | Possible causes of stridor at rest in previously well child |
|
| pharmacology | Prasugrel |
|
| neurology | Predictor of outcomes in TBI |
|
| cardiac | Predisposing conditions to VT / VF |
|
| trauma | Problems associated with the inability to clear the C-Spine include |
|
| trials | PROSEVA trial |
|
| pharmacology | Reasons for altered drug clearance in the critically ill include |
|
| renal | RIFLE criteria |
|
| infectious disease | Risk factors for C.difficile enterocolitis |
|
| infectious disease | Risk factors for development of VRE |
|
| haematology | Risk factors for tumour lysis syndrome |
|
| monitoring | Saefty features of ETT |
|
| statistics | Sensitivity |
|
| haematology | Short and long term effects of storage lesions |
|
| paediatrics | signs of 5 % and 10% dehydration in peadiatrics |
|
| trauma | Snakes which cause coagulopathy in Aus |
|
| statistics | Specificity |
|
| gastroenterology | Stages of Hepatic Encephalopathy |
|
| respiratory | Standard criteria for readiness for extubation include |
|
| haematology | Suggested criteria for activation of Massive Transfusion Protocol |
|
| organisational | The ideal scoring system would have |
|
| endocrine | The major biochemical abnormalities associated with Adrenal insufficiency include |
|
| biochemistry | The major biochemical abnormalities associated with tumour lysis syndrome include |
|
| statistics | the p value is | the probability the results have arisen by chance |
| equipment | Three chamber chest drain | 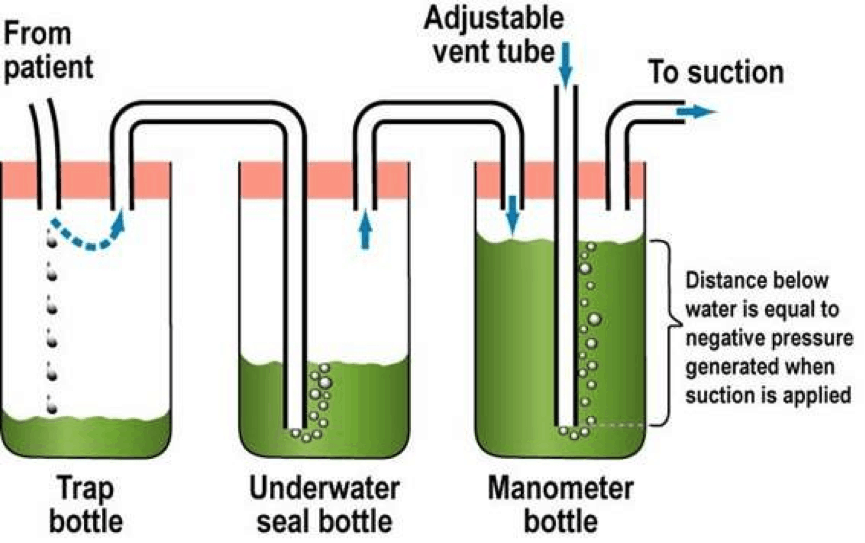 |
| trauma | three methods for estimating BSA affected by a burn |
|
| pharmacology | Ticagrelor |
|
| neurology | Time until clinical brain death testing can take place |
|
| toxicology | Toxicological causes of coma |
|
| trials | TracMan trial |
|
| statistics | Type 1 error (alpha error) is |
|
| statistics | Type 2 error (beta error) is |
|
| toxicology | Urinary alkalinization may be useful for poisoning with |
|
| monitoring | Uses of end tidal CO2 measurement in ICU |
|
| vasopressors | VASST trial |
|
| organ donation | Warm ischaemia time is |
|
| paediatric | Ways in which paediatric airways differ from adults include |
|
| renal | Ways of maximising urea clearance on RRT include |
|
| haematology | What are and what causes Howell Jolly bodies |
|
| pharmacology | what does 1/2 life determine |
|
| statistics | What factors affect the power of a study |
|
| statistics | What features to look for in a RCT to change your practice |
|
| statistics | What is the chi squared test | tests whether there is a real differnce in the frequency of categorical events between two or more groups |
| statistics | What is the likelihood ratio |
|
| trauma | What is the Parkland formula for burns |
|
| statistics | What is the Receptor Operator Characteristic curve | Plots sensitvity (y axis) against 1-specificty (equivalent to the false positive rate) (x axis) |
| nutrition | What is the respiratory quotient? | RQ= CO2 production (VCO2)/ O2 consumption (VO2) |
| nutrition | what is the Weir equation |
|


A third year advanced trainee in ICU at St Vincent’s Hospital Melbourne, completing dual fellowships in ICU and general medicine. At the moment I’m at Bendigo rotating through my anaesthesia term. I’ve completed the Fellowship exams in May this year with Maurice. Now my time is being filled by various research projects, exercising, eating out and wedding planning!

Advanced ICU trainee in Melbourne. Passed the fellowship examination in May 2014 with Sarah.









